
Project overview
The product
Banfield runs one of the largest networks of veterinary hospitals in the US, and its clinicians work inside a practice-management system that holds the patient, the visit, the medical record, and the orders. I worked on two modules within it: a nutrition recommendation engine and a medication/inventory flow, both used live, during an appointment, alongside everything else a vet is tracking.
The brief
Design clinical decision support that fits the existing software, not a separate tool. Smart Reco had to take a patient's clinical inputs and return the best-fit nutrition products with a rationale a vet could trust and share. The medication flow had to make prescribing, take-home or in-hospital, structured, validated, and fast.
Support the call, don't make it. Give the vet a fast, defensible recommendation and a structured way to prescribe, so the right decision is the easy one, without taking judgment out of their hands.
My role
I was a UX designer at Photon, the product studio working with Banfield, responsible for the Smart Reco and Inventory modules. I took both from wireframes through high-fidelity screens: the filter-to-recommendation flow, its empty and edge states, the shareable report, and the medication and ordering screens.
As with my later enterprise work, the discipline was designing inside an existing clinical system: respecting its dense, information-heavy layout and patterns while introducing decision support and structured prescribing the product hadn't had before.
A vet has minutes and two decisions that ran on memory
A vet in an exam has minutes, a talking client, and a patient who can't describe symptoms. Two recurring decisions, what to feed and what to prescribe, leaned heavily on memory and disconnected tools. The work was to make both faster and more consistent without adding clicks to an already busy screen.
Nutrition picked from memory
Recommending the right food meant recalling products across diagnoses, breeds, and conditions. Inconsistent, hard to justify, and easy to get wrong under time pressure.
Nothing to hand the owner
Even a good recommendation lived only in the vet's head or a quick note. Owners left without a clear plan, dosage, or transition schedule to follow at home.
Prescribing was unstructured
Medication, take-home vs in-hospital, dosing, refills, and ordering were fragmented. Without structure and validation, errors and omissions slipped through.
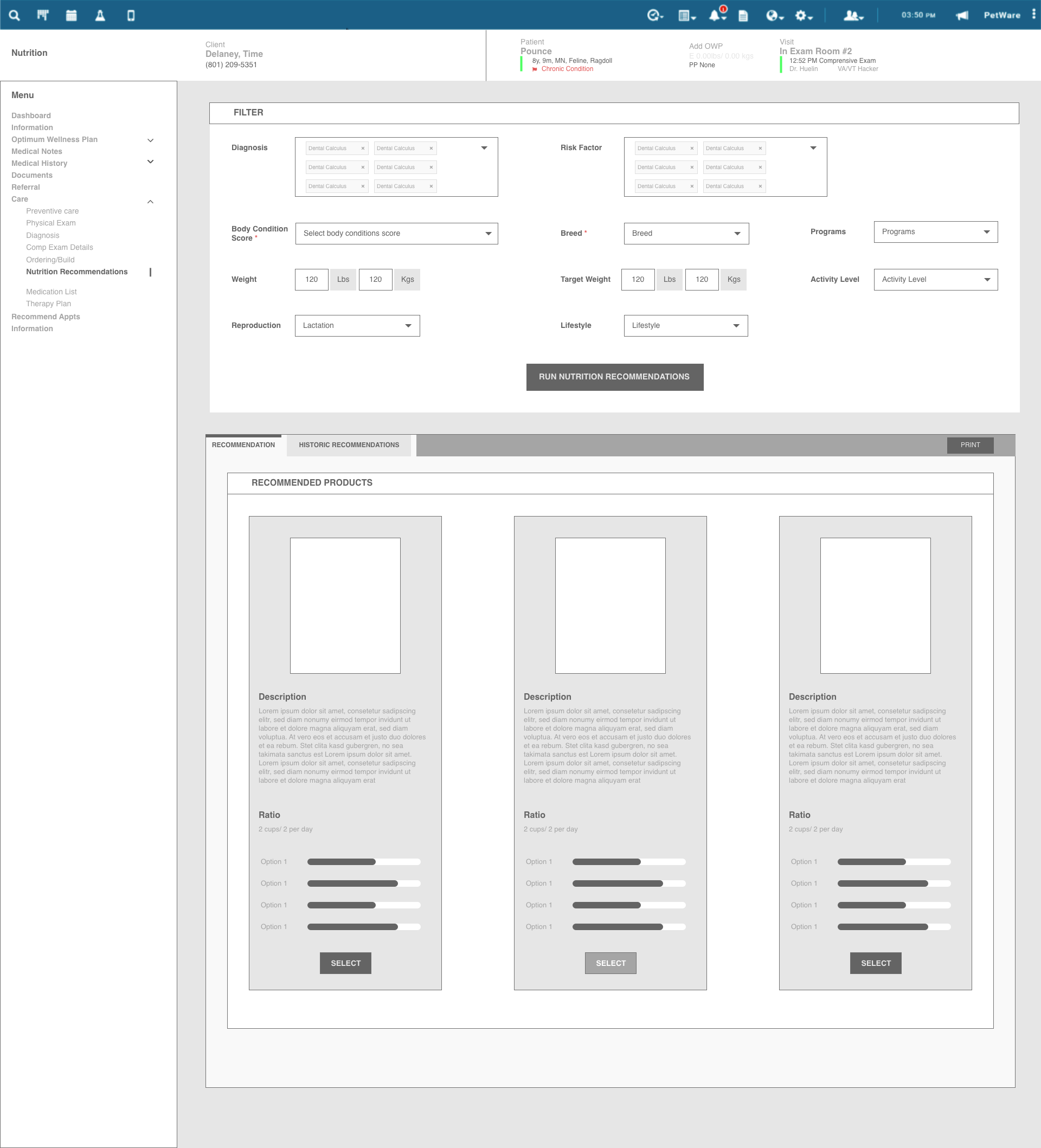
From wireframe to working screen
Smart Reco went through several iterations. I started in low fidelity to settle the hard question, what does a vet need to enter and how should three recommendations be presented and compared, before committing to the visual layer. The structure held; the polish followed.
Two modules, two decisions, both inside the practice system
Two modules, two decisions. Smart Reco answers "what should this animal eat?" from its clinical picture. The Inventory and medication flow answers "what am I prescribing, and how is it dispensed?" Both structured, both inside the practice software.
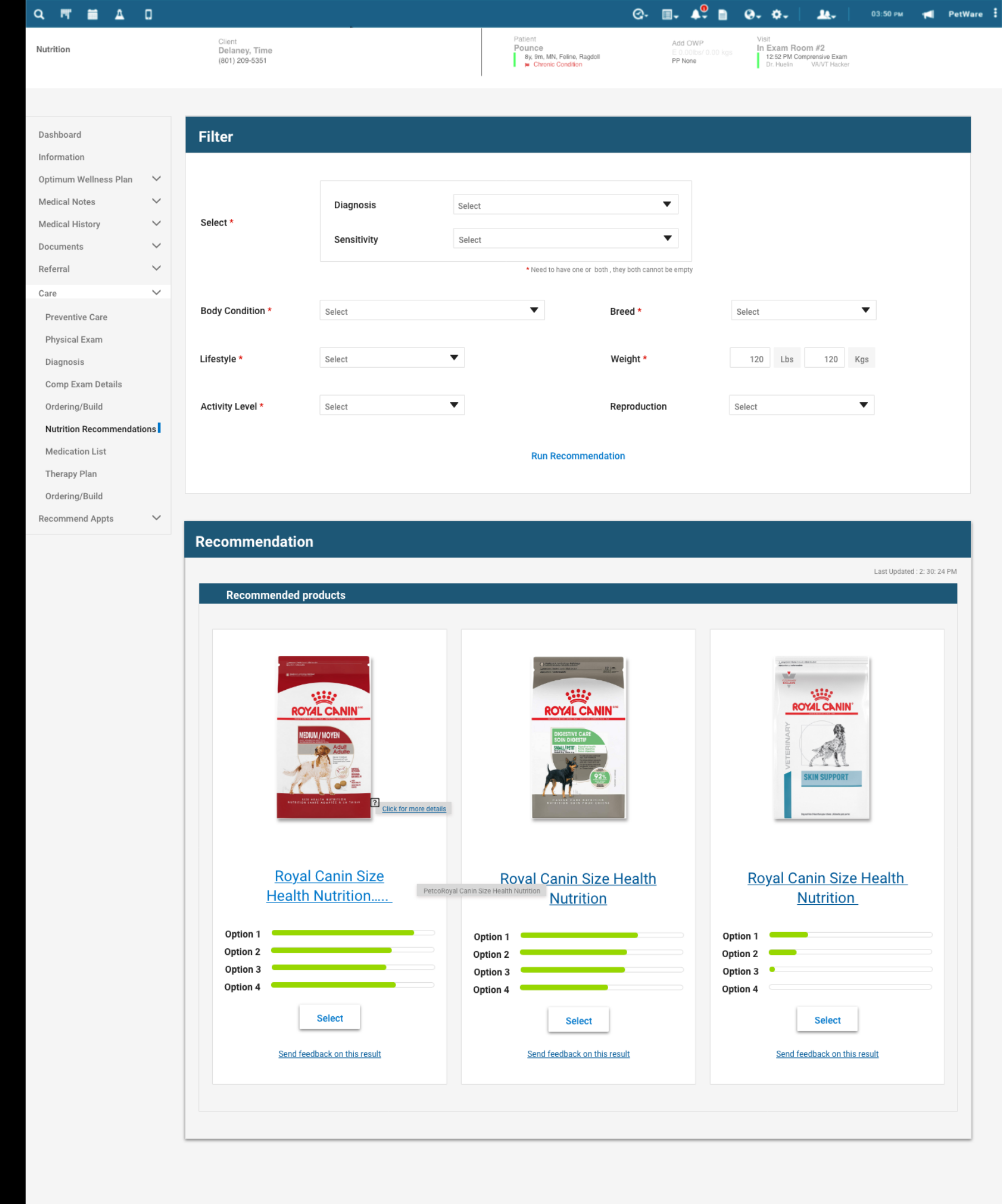
Clinical inputs in, top-three products out
The vet sets a patient's clinical picture: diagnosis, sensitivity, body condition, breed, lifestyle, weight, activity, reproduction, then runs the recommendation. Smart Reco returns the three best-fit nutrition products, each with a match breakdown so the vet can compare and choose, not just accept. It reads as part of the medical record, not a bolted-on calculator.
Why it matters: a memory task becomes a structured, comparable, defensible recommendation in seconds.
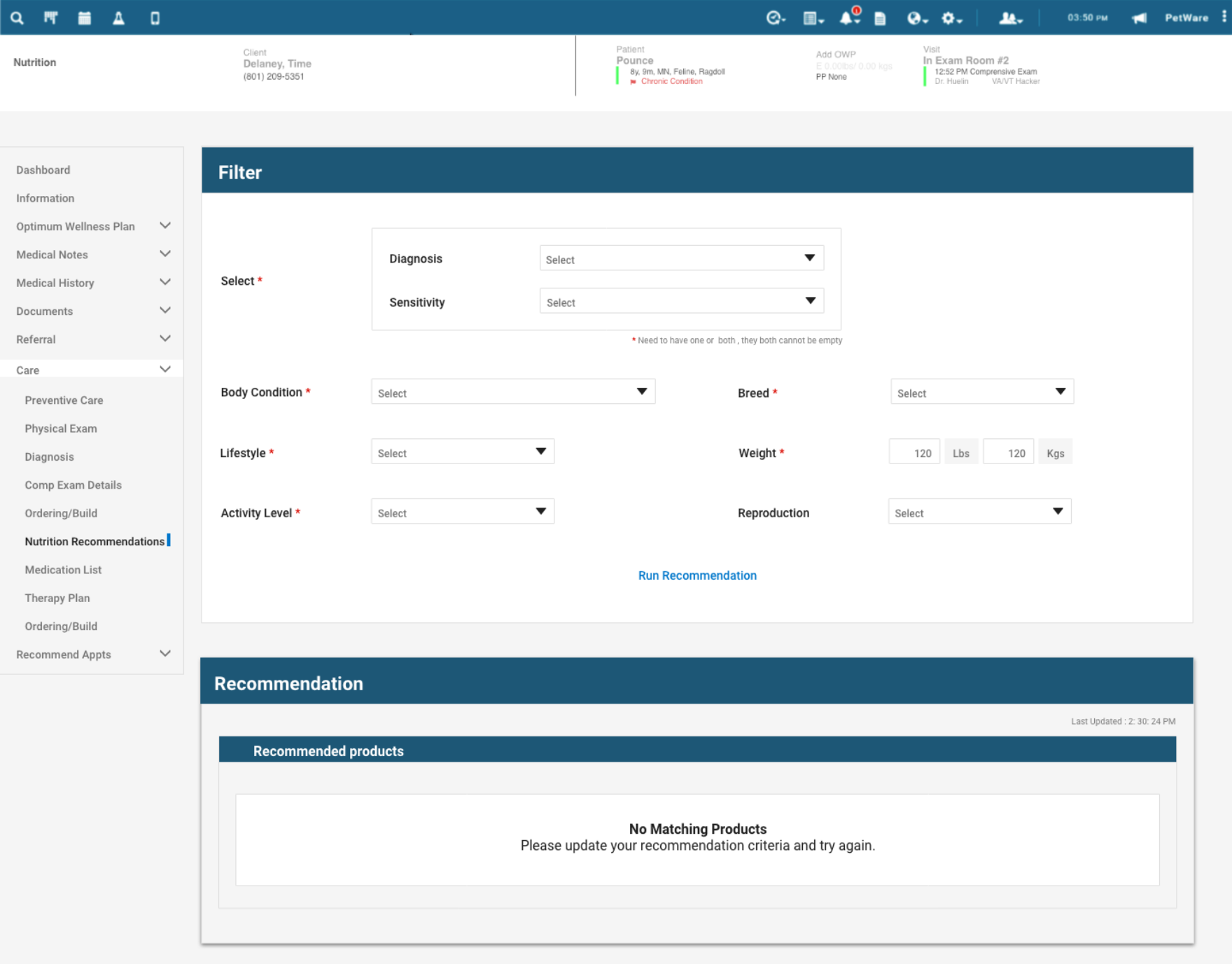
When nothing matches, say so clearly
Decision support must be honest about its limits. When no product matches the inputs, the screen says "No matching products" and asks the vet to adjust the criteria. Empty and edge states received the same attention as the happy path.
Why it matters: a clear "no answer" keeps the vet in control and the tool credible.
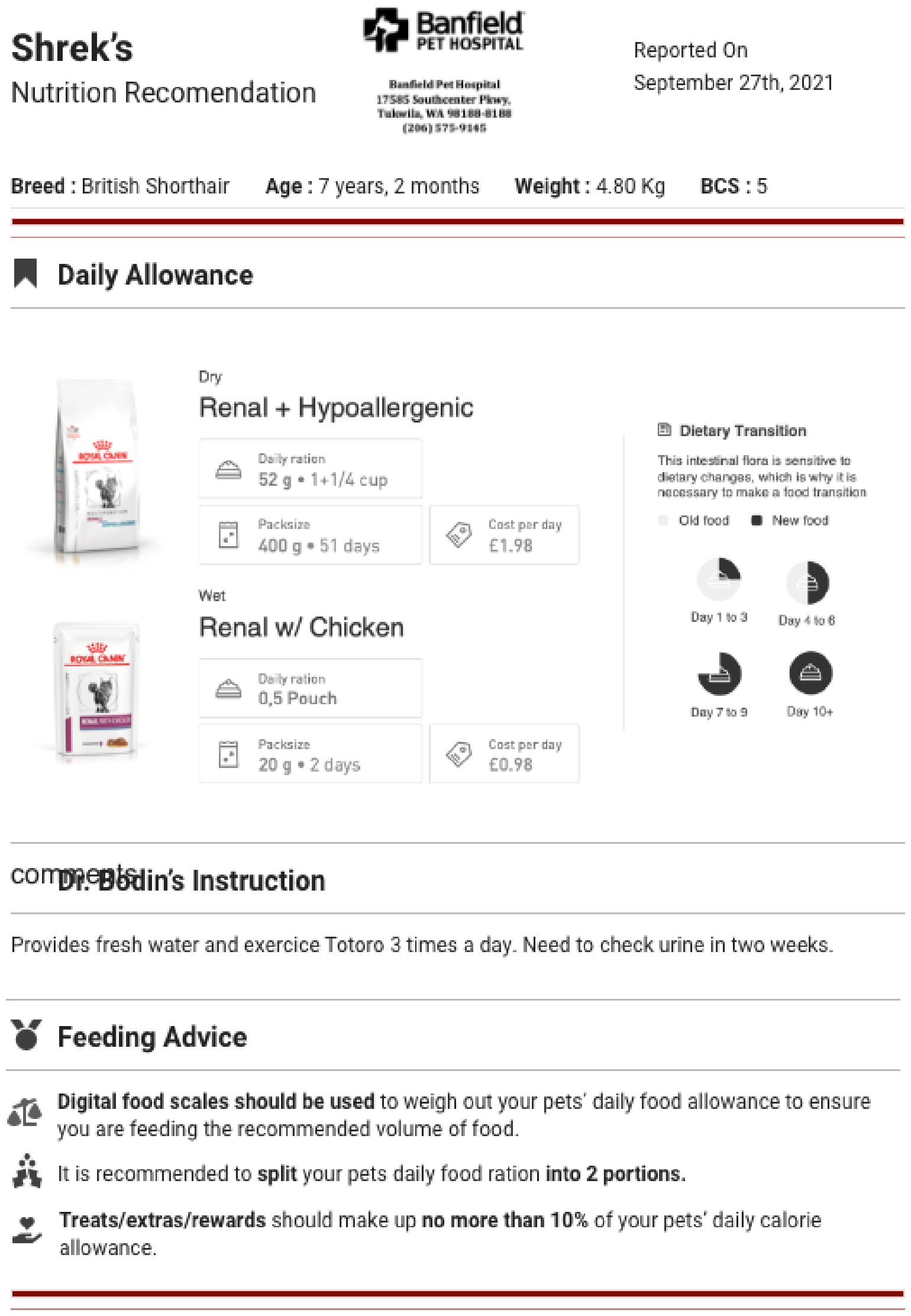
A report the owner takes home
The recommendation exports to a clean, branded PDF the vet can hand the pet owner: the chosen foods, daily allowance, a day-by-day dietary transition schedule, the doctor's instructions, and feeding advice. The decision leaves the exam room as a plan the owner can actually follow.
Why it matters: the recommendation becomes a take-home plan that helps owners follow through after checkout.
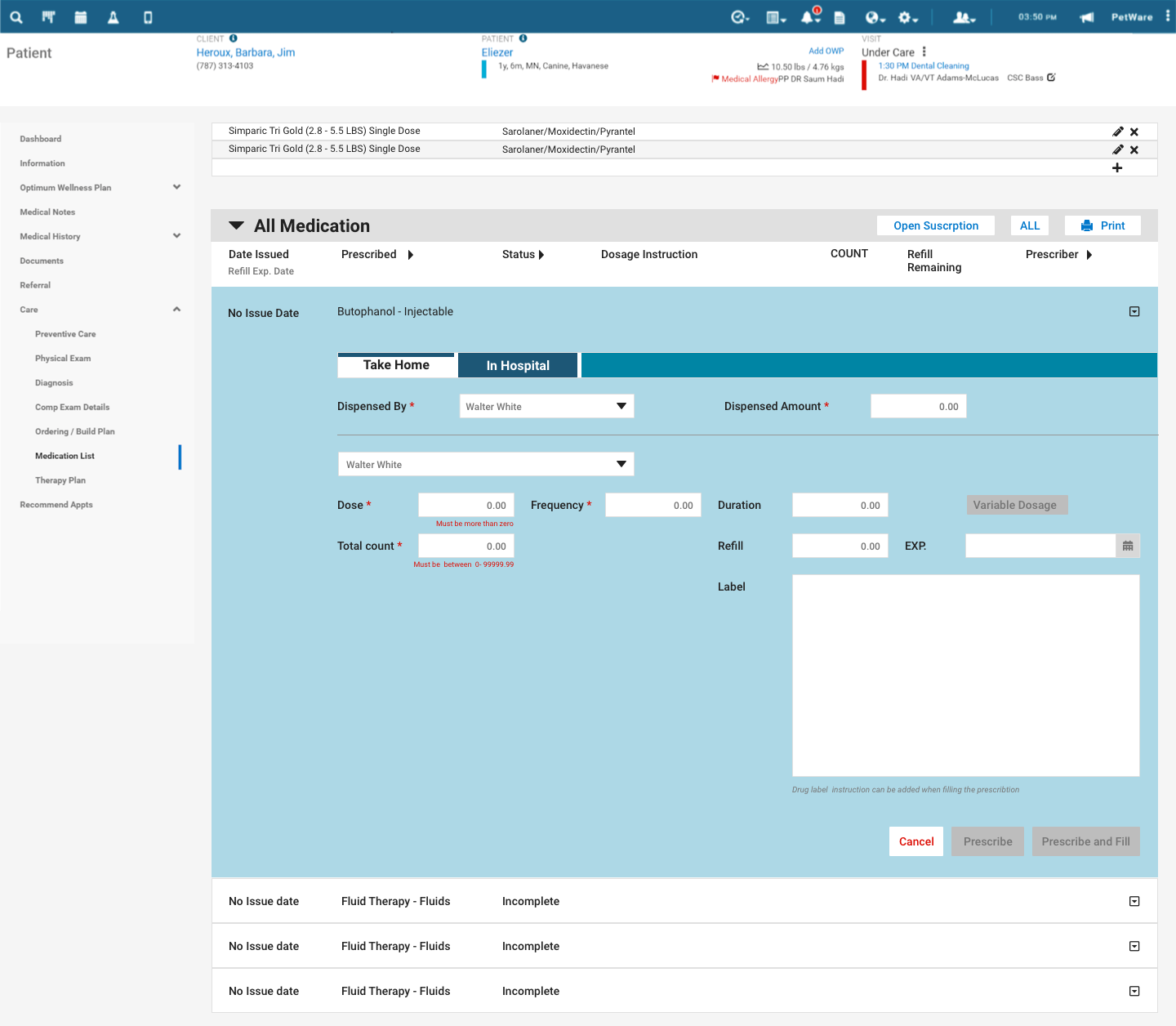
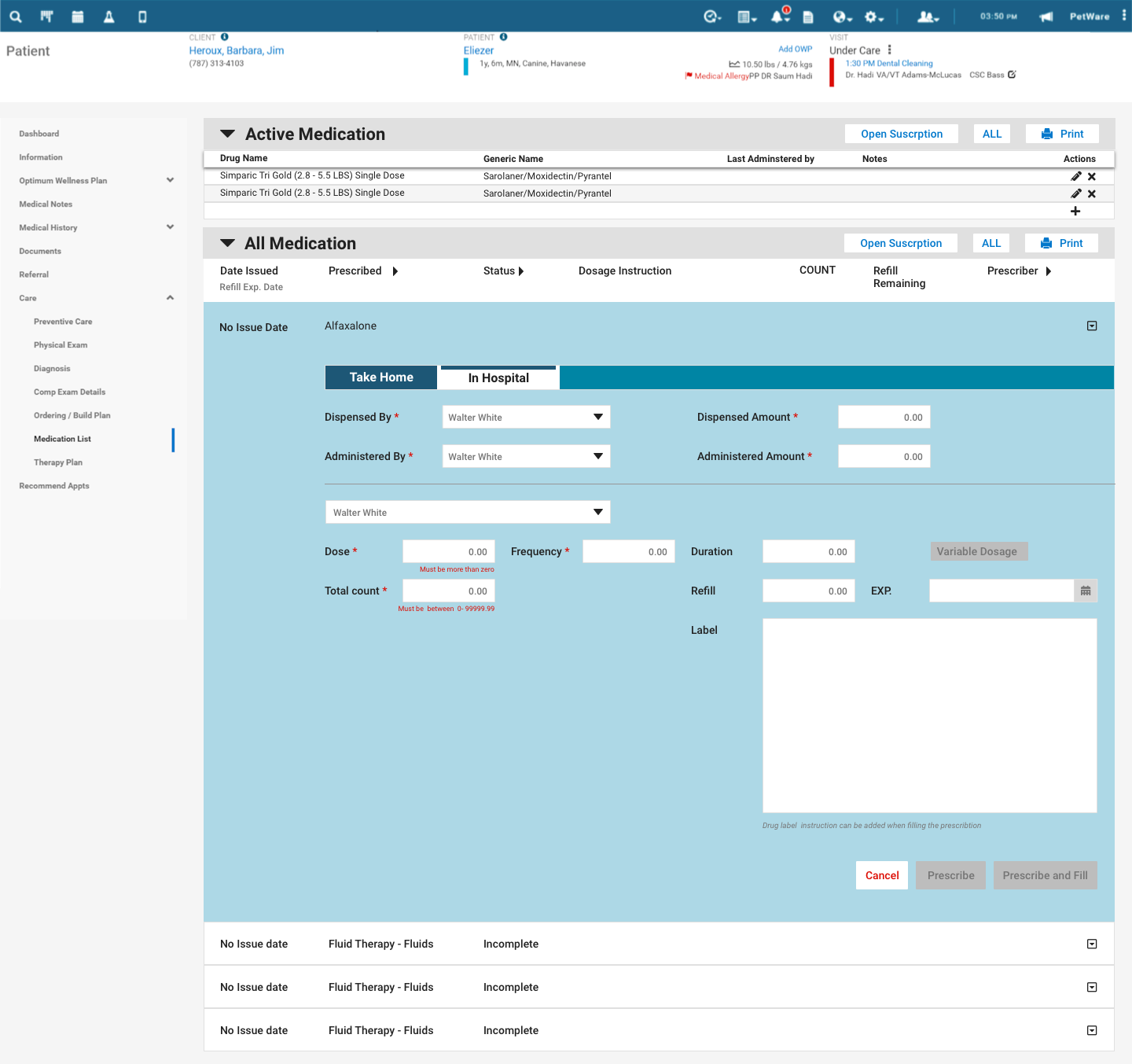
Prescribing, structured and validated
The medication flow keeps each prescription on one record. A Take-Home / In-Hospital toggle changes the context, while inline validation checks the dose, frequency, duration, refills, quantity, dispenser, and printed label before filling.
Why it matters: structure plus validation turns prescribing from a free-text risk into a checked, repeatable step.
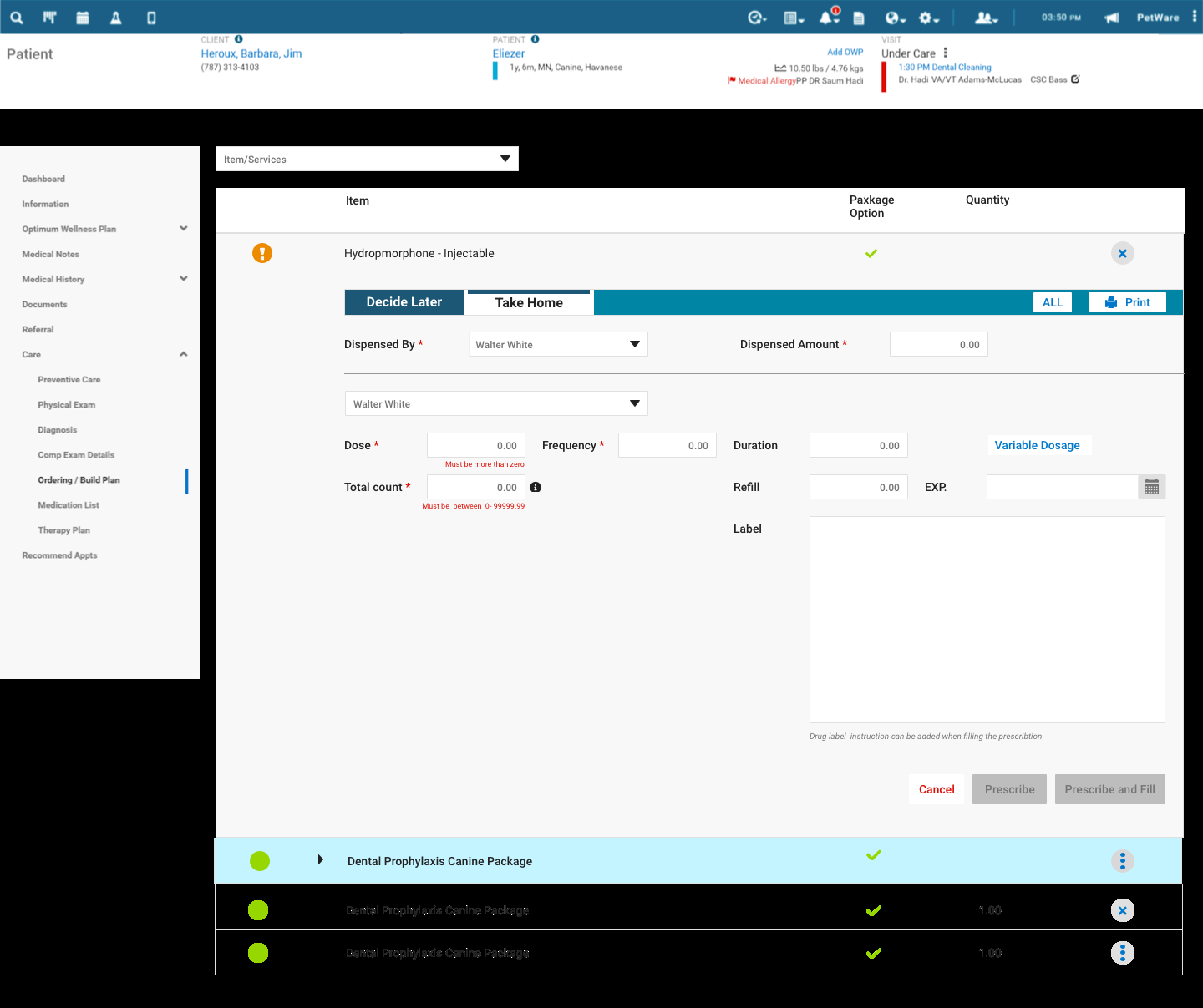
From prescription to ordering build plan
Prescribing connects to ordering: what's needed for the visit rolls into an ordering build plan, so stock and dispensing stay tied to the actual care given rather than tracked on the side. It closes the loop from the decision to the supply.
Why it matters: ordering reflects real care, so inventory and dispensing don't drift apart from what was actually prescribed.
Surface the rationale, keep the human in control
Decision support supports, never decides
The recommendation gives a vet three options and the reasoning, then gets out of the way. Same principle I'd later lean on for AI in financial systems: surface the rationale, keep the human in control.
Edge states are the real work
A clinical tool earns credibility by handling no-match results, validation errors, and take-home versus in-hospital cases clearly.
Wireframe the hard question first
Settling inputs and the three-up comparison in low fidelity, before any visual polish, is what kept the final screen coherent. Structure before surface.
Honest about the scope
This was early-career module work inside a large product, not the full research-to-impact arc. It's where the habits the rest of my portfolio is built on started to form.
Banfield taught me how to design for high-stakes, time-pressured work. Give clinicians a fast, defensible recommendation and a structured way to act, while keeping judgment and responsibility with them. I have carried that principle into every system I have designed since.